

‘Pedagogical Malpractice’: Inside UCLA Medical School’s Mandatory ‘Health Equity’ Class
Students in their first year of medical school typically learn what a healthy body looks like and how to keep it that way. At the University of California, Los Angeles, they learn that “fatphobia is medicine’s status quo” and that weight loss is a “hopeless endeavor.”
Those are two of the more moderate claims made by Marquisele Mercedes, a self-described “fat liberationist,” in an essay assigned to all first-year students in UCLA medical school’s mandatory “Structural Racism and Health Equity” class. Launched in the wake of George Floyd’s death, the course is required for all first-year medical students.
The Washington Free Beacon has obtained the entire syllabus for the course, along with slide decks and lecture prep from some of its most explosive sessions. The materials offer the fullest picture to date of what students at the elite medical school are learning and have dismayed prominent physicians—including those sympathetic to the goals of the class—who say UCLA has traded medicine for Marxism.
Jeffrey Flier, the former dean of Harvard Medical School and one of the world’s foremost experts on obesity, said the curriculum “promotes extensive and dangerous misinformation.”
UCLA “has centered this required course on a socialist/Marxist ideology that is totally inappropriate,” said Flier, who reviewed the full syllabus and several of the assigned readings. “As a longstanding medical educator, I found this course truly shocking.”
One required reading lists “anti-capitalist politics” as a principle of “disability justice” and attacks the evils of “ableist heteropatriarchal capitalism.” Others decry “racial capitalism,” attack “growth-centered economic theories,” and call for “moving beyond capitalism for our health.”
The essay by Mercedes “describes how weight came to be pathologized and medicalized in racialized terms” and offers guidance on “resisting entrenched fat oppression,” according to the course syllabus. Mercedes claims that “ob*sity” is a slur “used to exact violence on fat people”—particularly “Black, disabled, trans, poor fat people”—and offers a “fat ode to care” that students are instructed to analyze, taking note of which sections “most resonate with you.”
“This is a profoundly misguided view of obesity, a complex medical disorder with major adverse health consequences for all racial and ethnic groups,” Flier told the Free Beacon. “Promotion of these ignorant ideas to medical students without counterbalancing input from medical experts in the area is nothing less than pedagogical malpractice.”
Nicholas Christakis, a sociologist and physician at Yale University, who has spent decades providing medical care to underserved communities, including in the South Side of Chicago, called the curriculum “nonsensical.”
The relationship between health and social forces “should indeed be taught at medical school,” Christakis wrote in an email, “but to have a mandatory course like this—so tendentious, sloganeering, incurious, and nonsensical—strikes me as embarrassing to UCLA.”
UCLA did not respond to requests for comment.
Snapshots of the course have been leaking for months and left the school doing damage control as members of UCLA’s own faculty have spoken out against the curriculum. The most recent embarrassment came when a guest lecturer, Lisa Gray-Garcia, led students in chants of “Free, Free Palestine” after instructing them to kneel on the floor and pray to “Mama Earth.” Lessons on “decolonization” and climate activism, as well as a classroom exercise that separated students by race, have also stirred controversy.
“There are areas where medicine and public health intersect with politics, and these require discussion and debate of conflicting viewpoints,” Flier said. “That is distinct from education designed to ideologically indoctrinate physician-activists.”
The mandatory class is part of a nationwide push by medical schools to integrate DEI content into their curricula—for residents as well as students— both by adding required courses and by changing the way traditional subjects are taught.
Stanford Medical School sprinkles lessons on “microaggressions,” “structural racism,” and “privilege” throughout its curriculum. Residents at Yale Medical School must complete an “Advocacy and Equity” sequence focused on “becoming physician advocates for health justice,” while those in the infectious disease program must complete additional lessons on “Diversity, Equity, and Antiracism.”
Columbia Medical School promotes an “Anti-bias and Inclusive” curriculum by encouraging educators to use “precise, accurate language.” Instead of “women,” guidelines for the curriculum state, faculty should refer to “people with uteruses.”
The changes have been driven partly by the Association of American Medical Colleges—one of two groups that oversees the accrediting body for all U.S. medical schools—which in 2022 released a set of DEI “competencies” to guide curricula. Schools should teach students how to identify “systems of power, privilege, and oppression,” the competencies state, and how to incorporate “knowledge of intersectionality” into clinical decision-making. Students should also be able to describe “public policy that promotes social justice” and demonstrate “moral courage” when faced with “microaggression.”
The course at UCLA, which predates those accreditation standards, offers a preview of how DEI mandates could reshape medical education. It is littered with the lingo of progressive activism—”intersectionality” is a core value of the class, according to slides from the first session—and states outright that it is training doctors to become activists.
Students will “build critical consciousness” and move toward a “liberatory practice of medicine” by “focusing on praxis,” according to the slides.
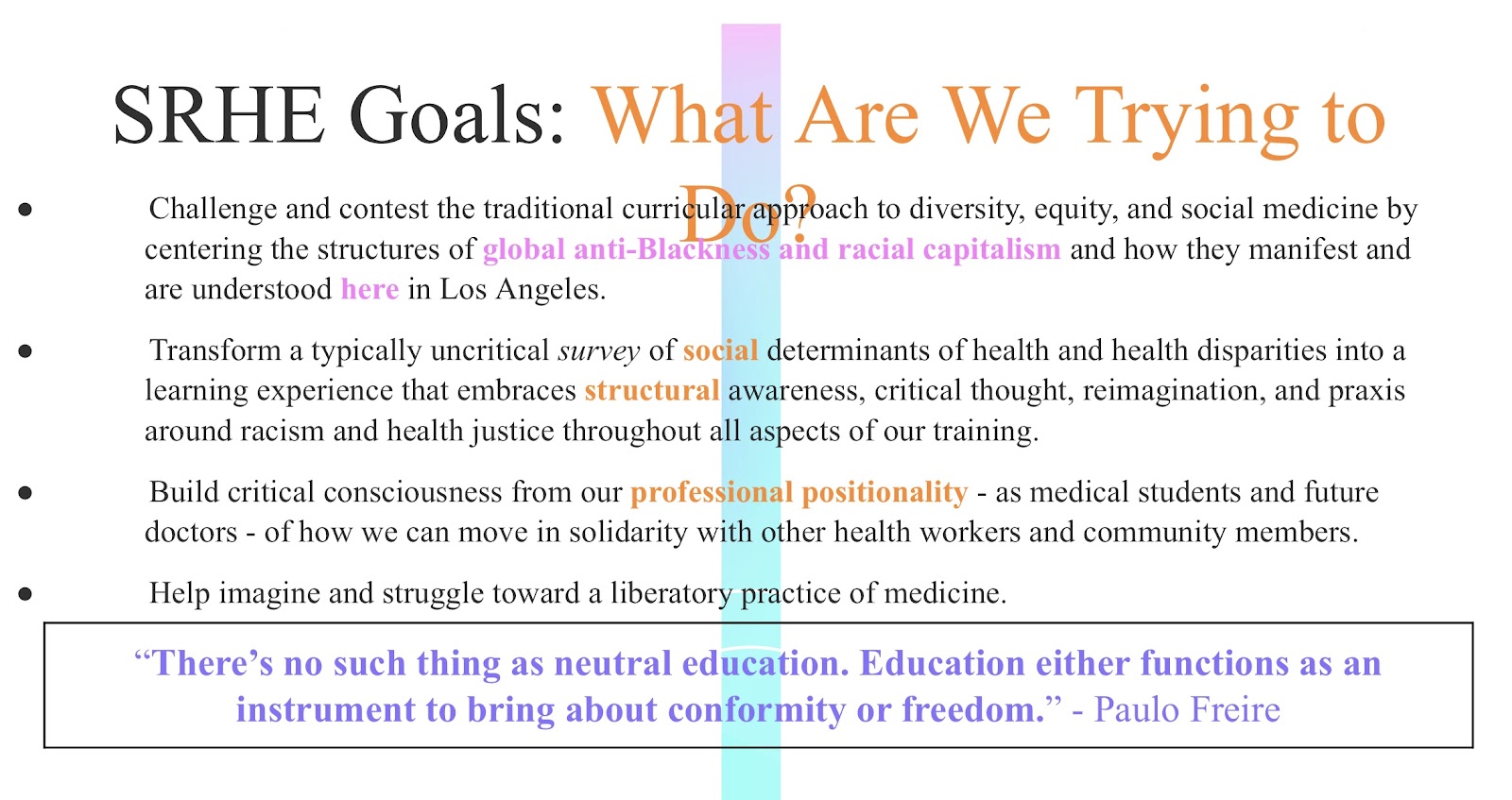
A section called “Our Hxstories” adds that “[h]ealth and medical practice are deeply impacted by racism and other intersectional structures of power, hierarchy, and oppression—all of which require humility, space and patience to understand, deconstruct, and eventually rectify.”
That jargon reflects a worldview with clinical implications. In a unit on “abolitionist” health, which explores “alternatives to carceral systems in LA,” students are assigned a paper that argues police should be removed from emergency rooms, where 55 percent of doctors say they’ve been assaulted—mostly by patients—and threats of violence are common, according to a 2022 survey from American College of Emergency Physicians. Other units discuss the “sickness of policing” and link “Queer liberation to liberation from the carceral state.”
Flier said the syllabus was so bad it called for an investigation—and that anyone who signed off on it was unfit to make curricular decisions.
“Assuming the school’s dean,” Steven Dubinett, a pulmonologist, “does not himself support this course as presented, it is his responsibility to review the course and the curriculum committee that approved it,” Flier said. “If that body judged the course as appropriate, he should change its leadership and membership.”
Dubinett did not respond to a request for comment.
One of the leaders of the course is Shamsher Samra, a professor of emergency medicine who in December signed an open letter endorsing “Palestinians’ right to return” and linking “health equity” to divestment from Israel.
“To authentically engage in antiracism health scholarship and practice is to explicitly name injustices tied to white supremacy and maintain an unapologetic commitment to antiracism praxis that transcends US borders,” the letter reads. “As such, we, the undersigned,* unequivocally support a free Palestine and Palestinians’ right to return.”
Samra, who in 2021 published a paper on “infrastructural violence and the health of border abolition,” did not respond to a request for comment.
To the extent the course addresses actual medical debates, it frames contested treatments as settled science, omitting evidence that cuts against its activist narrative. A unit on “Queerness/Gender,” for example, assigns readings on “gender self-determination” and “DIY transition,” but does not include any of the research from Europe—such as the newly released Cass Report—that has led England and other countries to restrict hormone therapies for children.
“UCLA School of Medicine has decided to shield its students from the ongoing scientific debates playing out in Europe and even in the U.S.,” said Leor Sapir, a fellow at the Manhattan Institute who researches gender medicine. “This is fundamentally unserious, and a stain on the school’s reputation.”
The omission of inconvenient facts extends to a unit on Los Angeles’s King/Drew hospital—nicknamed “Killer King” for its high rates of medical error—which the course promotes as an example of “community health.”
Founded in 1972 as a response to the Watts riots, the hospital was majority black, had a documented policy of racial preferences, and was hit with several civil rights complaints by non-black doctors alleging discrimination in hiring and promotion.
It closed in 2007 after a Pulitzer Prize-winning investigation by the Los Angeles Times found numerous cases in which patients had been killed or injured by clinical mistakes, such as overdosing a child with sedatives and giving cancer drugs to a meningitis patient. Efforts to reform the hospital stalled, according to the Times, because its board of supervisors feared coming across as racially insensitive.
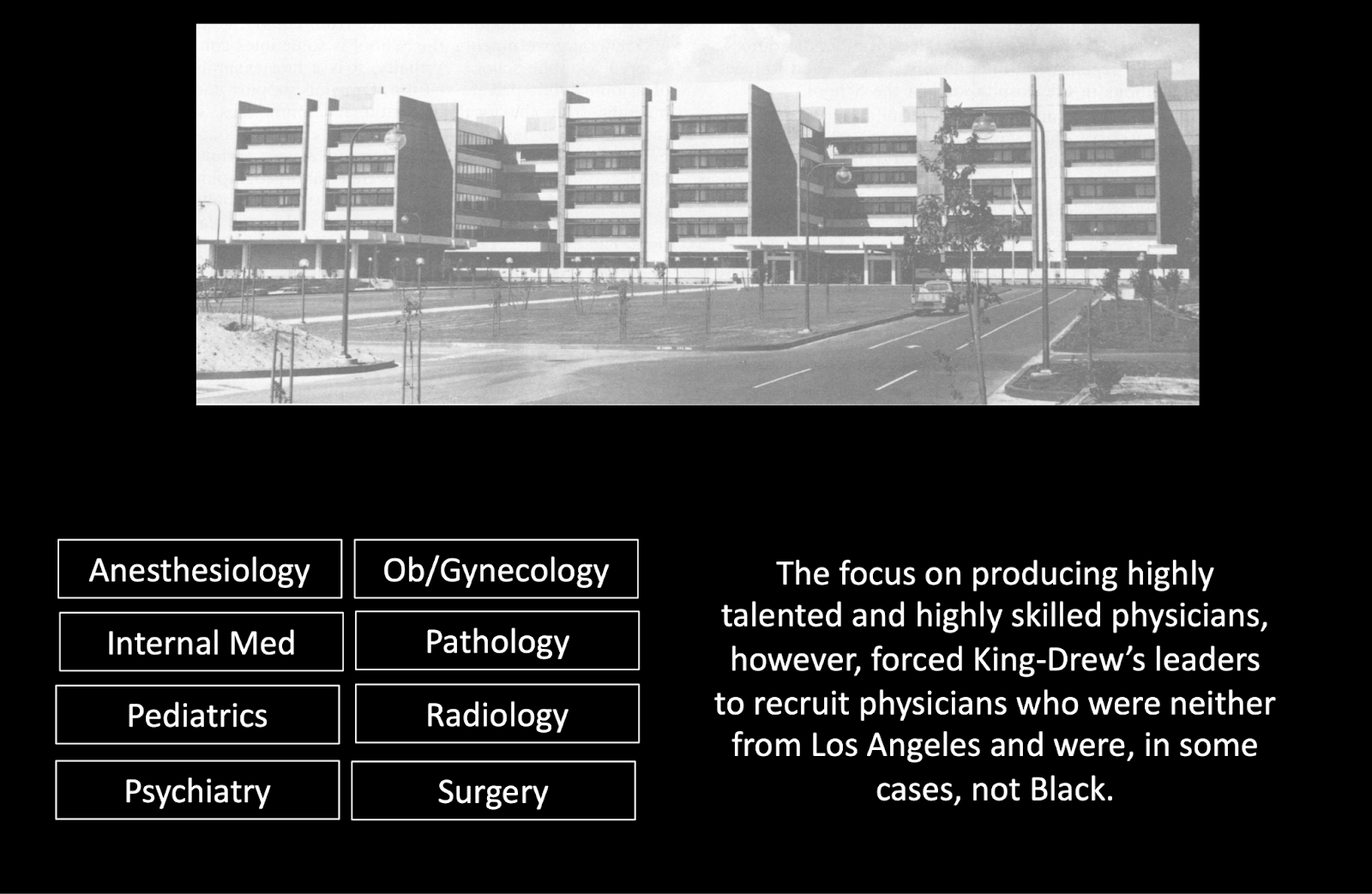
The assigned readings on King/Drew do not include any of this history. Lecture slides instead praise the hospital for “suturing racial divides,” but suggest that it may not have gone far enough. A focus on “producing highly talented and skilled physicians,” one slide reads, “forced” King/Drew to hire doctors who were, “in some cases, not Black.”
The curriculum is a “compilation of ideologic and anecdotal assertions that represent a warped view of medicine,” said Stanley Goldfarb, the founder of the medical advocacy group Do No Harm and the father of Free Beacon chairman Michael Goldfarb. “American medical education needs to purge itself of this nonsense and treat every patient as an individual.”
The slides suggest that “lived experiences,” “historical memory,” and “other knowledges” can constitute medical expertise.
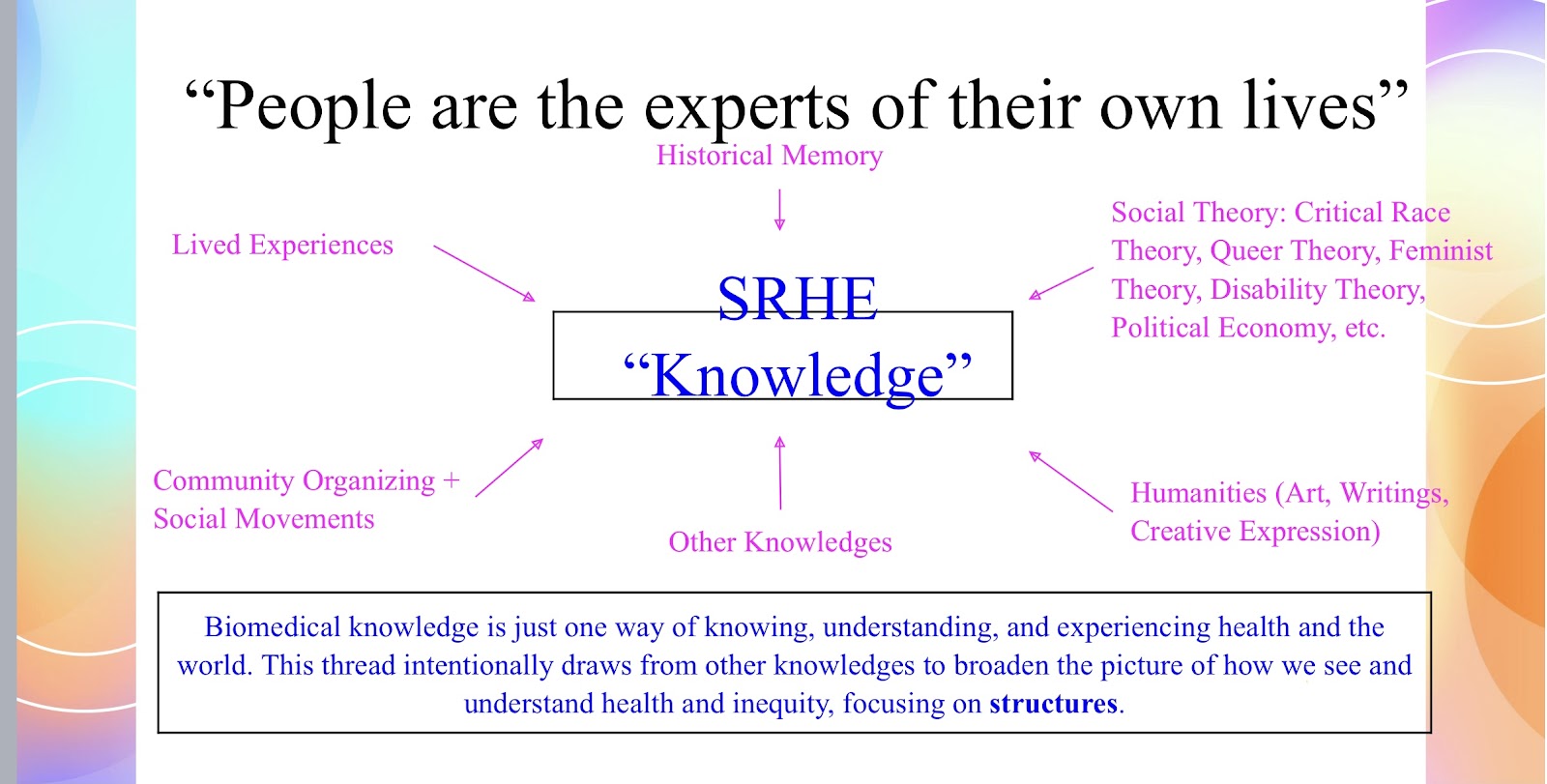
Biomedical knowledge, after all, is “just one way of knowing, understanding, and experiencing health in the world.”