

The Disturbing Historical past of Vaccine “Hot Lots”
The following information is based on a report originally published by A Midwestern Doctor. Key details have been streamlined and editorialized for clarity and impact. Read the original report here.
You’ve probably heard this more times than you can count:
“I got the COVID vaccine and nothing bad ever happened to me.”
There’s a reason for that… not everyone got the same thing.
And a peer-reviewed study backs it up.
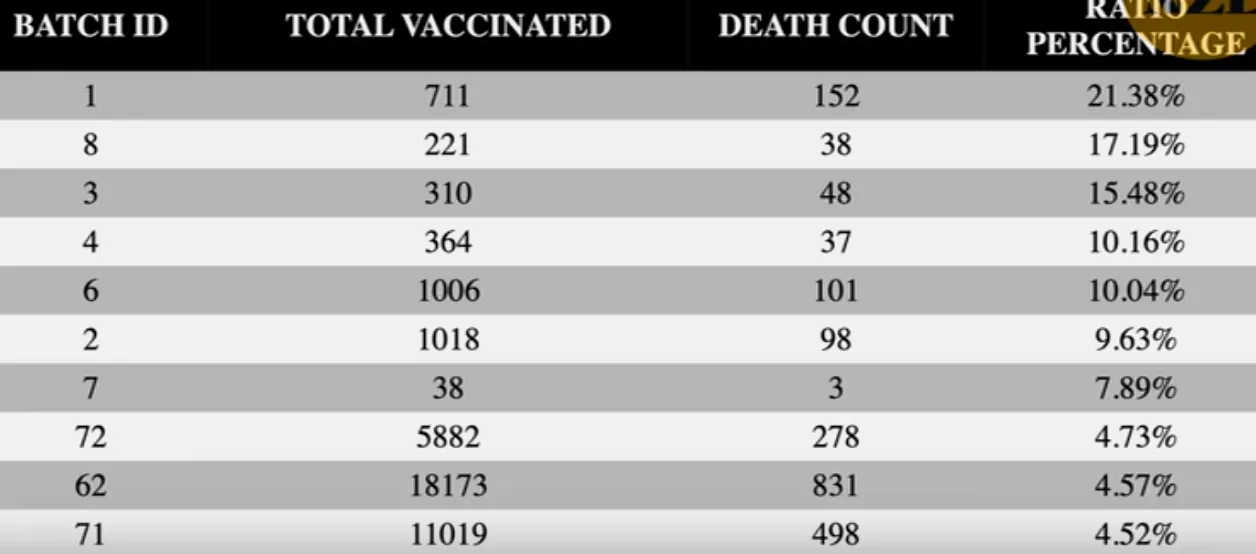
In 2023, Max Schmeling and colleagues discovered that just 4.2 percent of the COVID vaccine batches accounted for 71 PERCENT of suspected adverse events.
Additionally, about two-thirds of the batches had a low to moderate risk of adverse events.
And about one-third had little to no risk of adverse events. “Nothing happened.”
The chart below shows how extreme this variation actually was.
“The shot [batch] was deterministic for who was going to have a serious event or not.” That’s the conclusion from renowned cardiologist Dr. Peter McCullough.
If “hot lots” showed up in the COVID shots, that raises a bigger question about other vaccines.
What if this wasn’t a one-time issue? Let’s take a look.
For over a century, one assumption has quietly shaped public trust:
If a vaccine is approved, what’s in each vial must be safe and consistent.
Same dose. Same safety. Same outcome.
But history tells a very different story.
Because again and again, the real danger wasn’t always the vaccine itself… Sometimes it was the batch.
This information comes from the work of medical researcher A Midwestern Doctor. For all the sources and details, read the full report below.

There’s a term most people have never heard: “Hot lots.”
It refers to vaccine batches that are unusually toxic, contaminated, improperly processed, or far more likely to cause severe reactions than other lots.
And once you start looking, they don’t appear once. They appear everywhere.
This isn’t a modern controversy.
It’s a pattern stretching back more than 100 years.
Different countries. Different vaccines. Different technologies.
But the same dangerous situation: One batch behaves normally, another batch… doesn’t.

Early vaccine production had a fundamental problem.
These weren’t simple chemical pills.
They were biological products—grown, cultured, handled, purified.
Which means there were multiple failure points.
Things like contamination, incomplete inactivation, toxin residue, and dose inconsistency.
And when those failures made it into vials, they didn’t affect everyone equally—they clustered.

What makes this topic so unsettling isn’t one event. It’s how often the same pattern shows up across decades—from early childhood vaccines to military programs to COVID-era data.
The full breakdown from A Midwestern Doctor goes far deeper than what most people have ever seen.
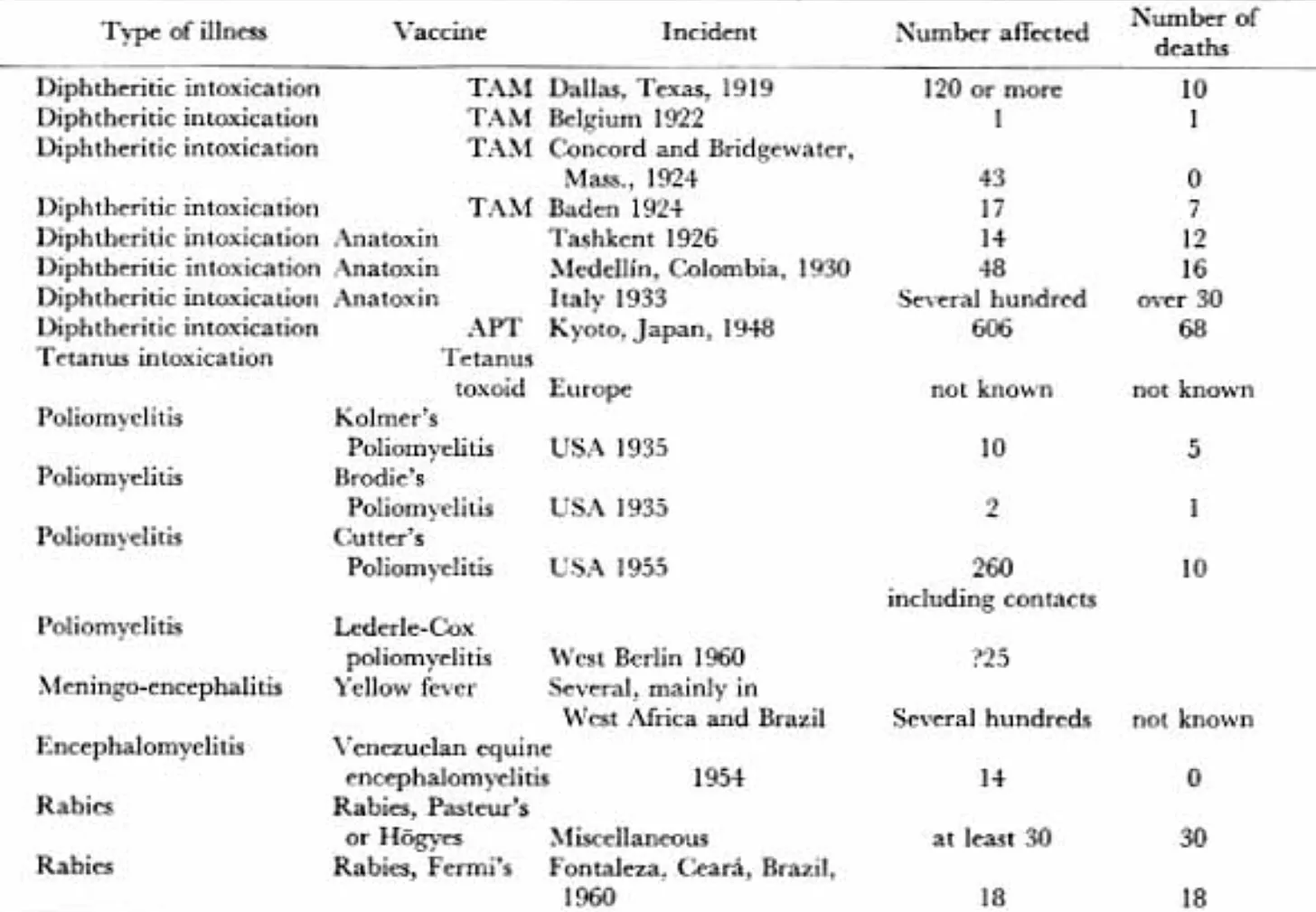
For example, take Dallas in 1919.
A diphtheria campaign used multiple lots.
One of them contained over 50 times the maximum permissible level of free diphtheria toxin.
Of 120 children later studied, 96 had reactions, 74 were severe, and 10 died.
But those numbers don’t capture the reality that those affected had to live with.

The progression was brutal.
It started with intense burning at the injection site.
Then nausea. Vomiting. Massive swelling.
Within days, blistering wounds formed—leaking fluid and leaving raw tissue behind.
Then came heart irregularities. Then paralysis.
Not for hours. For weeks.
Some symptoms lasted 4–5 months.

And Dallas wasn’t an outlier.
Belgium. Massachusetts. Colombia. Italy. Japan.
Again and again, specific batches caused disproportionate harm.
In Kyoto in 1948, over 600 infants and children became ill from one lot, and at least 68 died.
Same underlying issue: Toxin that was supposed to be neutralized wasn’t.

This is where the pattern becomes undeniable.
These weren’t random adverse events.
They were clustered reactions tied to specific lots.
Same product. Same protocol.
Completely different outcomes depending on the batch.

Then came polio.
One of the most celebrated public health victories.
But buried inside that story is one of the largest medical failures in history.
The Cutter incident of 1955.
A vaccine meant to contain an inactivated virus.. didn’t.
At least 220,000 people were infected, 70,000 developed muscle weakness, 164 were severely paralyzed, and 10 died.
All from a product that was supposed to be safe.

The lesson here should have been permanent and it should have inspired action.
Manufacturing failure isn’t theoretical. It’s catastrophic.
It doesn’t always show up evenly. It shows up in clusters.
And it shows up in lots.

The early disasters alone are enough to challenge the idea of consistency in vaccines. But things take a darker turn when you get into infant vaccine clusters, military programs, and modern rollout data.
Then came the BCG disaster in 1929.
A tuberculosis vaccine was accidentally contaminated with live TB bacteria.
251 infants received that vaccine. 72 of them died and 135 became ill.
Only 44 showed no symptoms.

But this time, something different happened.
There were trials and investigations.
And even prison sentences.
Accountability existed—at least briefly.
That detail matters more than it seems, because later cases didn’t follow that pattern.
Earlier disasters sometimes led to trials and accountability.
Later ones too often ended in ambiguity, delayed action, or silence.

Fast forward to DPT.
By the 1970s, internal warnings were already clear.
One FDA official described it as “one of the more troublesome products to produce.”
Lot-to-lot variability wasn’t rare, it was expected.
And one safety study made that even harder to ignore.
In 1978, researchers found adverse reactions within 48 hours of DPT vaccination were 5000% higher than expected.
The study was ended early.
Those findings never made it into the final publication.

Between August 1978 and March 1979, 11 infants in Tennessee died within 8 days of vaccination.
Four of them died within 24 hours.
They all received the same lot. Wyeth lot #64201.
These weren’t statistical anomalies. They were infants—clustered in time, tragically linked by a lot number.

And that wasn’t the only red flag.
In 1975, the FDA denied approval of a DPT batch after determining it was 300% too potent.
But state officials disagreed.
So they tested it on children. Then released 400,000 doses statewide.
Here’s where things get complicated.
Even with a clear cluster, officials said a causal relationship had not been established, while also admitting it could not be totally excluded.
That gray zone and inability to commit becomes a recurring theme.

Behind the scenes, another idea emerged.
A Midwestern Doctor reveals internal Wyeth correspondence showing that if dangerous lots couldn’t be avoided, the practical response became spreading them around geographically so the pattern would be harder to see.
If bad lots are unavoidable, don’t concentrate them. Distribute them!
That means less clustering, less visibility, and no accountability.

What looks like a disappearance of dangerous clusters might actually be a change in distribution strategy.
The full article from A Midwestern Doctor connects that pattern to modern data.
This same pattern doesn’t stop with civilian vaccines.
It happened in the military, too.
The anthrax program during the Gulf War raised similar concerns.
Not just about side effects—about manufacturing, too.

At one point, the manufacturer reportedly switched to larger filters that didn’t clog as easily.
But they were also less effective at purification.
Meaning more contaminants could pass through.
Better for production efficiency, but worse for purification and for recipients.

And that brings us to now—the modern era of vaccines.
Now we have a completely new platform—mRNA.
But it was rushed to global scale under extreme pressure.
If we look at history, there are obvious questions that should be asked about this.
The challenge with this new process isn’t just biology. It’s consistency.
Maintaining stable mRNA
Preventing degradation
Ensuring uniform nanoparticle distribution
Avoiding contamination
All on an absolutely massive scale under the most intense time pressure.
Is there any chance something went wrong?

What has emerged since hasn’t been a smooth spectrum of reactions.
It’s been uneven.
Some people had no reaction at all.
Others had severe outcomes.
That kind of distribution raises a very specific question: Was every dose actually the same?

Independent analyses began pointing to something familiar. Something we’ve seen before.
What those analyses suggested was striking.
In some datasets, almost all reported vaccine deaths were linked to roughly 5% of the lots.
Not evenly distributed. Not random.
Concentrated.
A modern echo of an old pattern.
From early toxin failures to polio, infant clusters, military programs, and modern rollouts—the same structural issue keeps resurfacing.
Not just whether an injection is safe.
But whether it’s consistent.
And what happens when it isn’t… when the risk isn’t evenly shared.

Thanks for reading! This information was based on a report originally published by A Midwestern Doctor. Key details were streamlined and editorialized for clarity and impact. Read the original report here.
For a deeper dive into what modern medicine has overlooked—or intentionally buried—check out these other eye-opening reports by A Midwestern Doctor:
The Forgotten Cancer Cure Hiding in Plain Sight
What They Don’t Tell You About C-Sections
What’s The Healthiest Water To Drink?
While you’re at it, give A Midwestern Doctor a follow. No one brings more research, clinical insight, or historical context when it comes to exposing the health myths we’ve all been fed. This is easily one of the most valuable accounts you’ll ever follow.

If you haven’t subscribed to this Substack yet, take a moment to read what some of the most powerful voices in the medical freedom/truth movement have to say:
“The Vigilant Fox has been putting in a lot of work to create a news platform that shares the stories we want to hear about and brings attention to the most important things to know about. If you want a daily newsfeed in alignment with our …”
– A Midwestern Doctor, The Forgotten Side of Medicine
“The Vigilant Fox absolutely is on top of things. We must support our fighters, and the Fox is fighting with truth.”
– Tom Renz, Tom Renz’s Newsletter
“Excellent capture of key video presentations on evolving pandemic science.”
– Peter A. McCullough, MD, MPH, FOCAL POINTS (Courageous Discourse)